- Customer Care +91 8800900271
- About Us
- Contact Us
- Sell Your Brand
- International Orders

Use Your Social Media Account
Google|| Shake The Bottle, Remove The RINGWORM ||
- By: Dr Preeti Kumari
- Profession: BHMS
- Category: Homoeopathy
- Jan 18, 2021
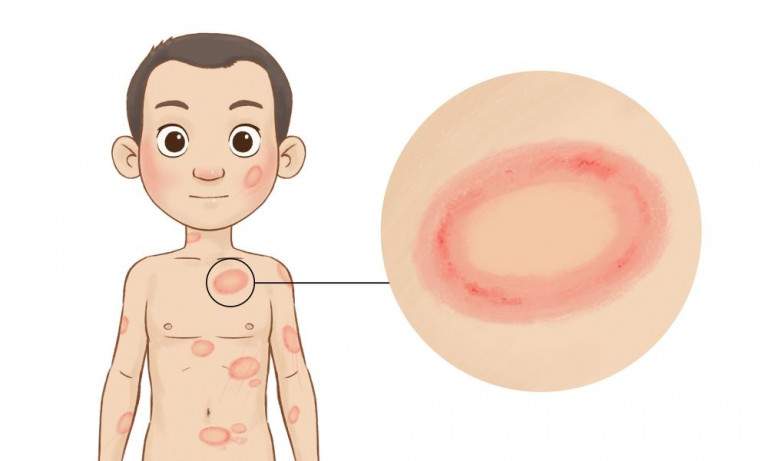
Ringworm is a common fungal skin infection otherwise known as tinea. Ringworm most commonly affects the skin on the body, the scalp, the feet, or the groin. It is highly contagious.

Typically, it appears as a ring-shaped rash. It can have a red center or clear center and an active margin with papulovesicles and scaling.
Three genera of dermatophytes infect skin.
- Trichophyton
- Microsporum
- Epidermophyton
Dermatophytes are keratinophilic fungi and have the ability to invade keratinized tissue. They invade, infect and persist in the stratum corneum of the epidermis and rarely penetrate below the surface of epidermis and its appendages.
They induce inflammation of skin due to
- Permeation of their metabolic products into deeper tissue
- Induction of delayed hypersensitivity
Humid and moist skin provides a very favorable environment for the establishment of fungal infection.
- It is an annular or arcuate lesion which spread centrifugally.
- The margin is active showing papulovesiculation, pustulation, and scaling
- Centre is relatively clear
- In chronic lesion there may be nodules, hyperpigmentation and even lichenification in the center.
- The features may be modified, depending upon
A) Site of infection
B) Strain of fungus
- Summer and rainy season
- Living in a warm climate
- Contact with infected person or animal
- Sharing clothing, bedding, or towels who have fungal infection
- Wearing tight or restricted clothing
- Communal baths
- Have a weak immune system
.png)
1. TINEA CAPITIS

- Tinea of scalp
- Caused by: Microsporum and Tricophyton
- One or more round patches from where hair can be easily and painlessly plucked out
- Three patterns are recognized
- Non-inflammatory tinea capitis

- Appear as partially bald areas with scaling most marked in periphery
- Hair present in patches are lusterless, may break 3-4 mm from the scalp and can easily be plucked.
- The broken hair may appear as gray/black dots.
- Inflammatory Tinea Capitis (kerion)

- Present as boggy swelling with pustulation
- The pus discharges from multiple orifices
- Hair from such swelling can be easily and painlessly plucked
- Lymph nodes may be enlarged
- Favus: Characterized by presence of foul-smelling yellowish cup shaped crusts entangling many scalp hair

- TINEA CORPORIS:

- Tinea of trunk and limbs.
- Lesions with relative clearing in the center and an active periphery
- TINEA CRURIS (JOCK ITCH)

- Tinea of groin
- A very common condition
- Seen on the inner aspect of thighs as sharply demarcated plaques with peripheral scaling
- TINEA PEDIS (ATHLETE’S FOOT)

- Usually begins between the toes
- It commonly occurs in people who have:
~ Occlusive foot sweat
~ Hyperhidrosis of soles
- TINEA MANNUM:Tinea of hands.

- TINEA UNGUIUM: Tinea of nails

*TINEA INCOGNITO: Dermatophytic infection of skin modified by steroid therapy.
Atypical lesions, usually asymptomatic, poorly defined edge with minimal scales and papulovescicles.
- Keep your skin clean and dry.
- Wear shoes that allow air to circulate freely around your feet.
- Change your socks and undergarments daily
- Don’t share clothing, towels, sheets or other personal items.
- Wash your hands with soap and running water after playing with pets.
- TUBERCULINUM: Ringworm like eruptions all over body. Itching intense. Aggravation at night when undressing. Immense quantities of white bran like scales. Ringworm in folds of skin with rawness and soreness. Fiery red skin. The patient perspires much. Person is chilly and takes cold easily. The person is tall, slim, flat, narrow chested and have tubercular diathesis. Active and precocious mentally and weak physically.
- ACID CHYRSOPHANICUM: Acts as powerful irritant of the skin and is used successfully in skin diseases, especially in ringworm. Vesicular or squamous lesions, associated with foul smelling discharge and crust formation. Violent itching of the parts affected.
- TELLURIUM: Ring shaped lesions on the body. Itching of the affected parts. There is stinging in the skin. Offensive discharges from the eruptions. Fetid exhalations. Offensive foot sweat. Circular patches of eczema on skin. Barber’s itch.
- SEPIA: It acts wonderfully in ringworm. Ringworm in isolated spots on upper part of the body. Itching not relieved by scratching. Ringworm like eruptions in every spring. Dry ringworm on face. Relief from warmth of bed, hot applications. Worse in bends of elbows and knees. Offensive odor of skin.
- SULPHUR: Skin affections that have been treated with medicated soaps and washes. Skin eruptions with intense itching. Feels good to scratch. Scratching causes burning. Aggravation from heat of bed. Soreness in folds. Skin excessively sensitive to atmospheric changes. Skin is dry, scaly and unhealthy.
- PSORINUM: Skin looks dry, lusterless and dirty. Intolerable itching. Eruptions on the scalp and in bends of joints with itching. Crusty eruption all over. Body has filthy smell even after bathing. Great sensitiveness to cold air. Dry scaly eruption disappears in summer and return in winter. Skin looks greasy as if bathed in oil. Bad effects from suppression by sulphur and zinc ointments.
- NATRUM MURIATICUM: Often useful in herpes circinatus. Face of the patient is pale, shining, greasy looking. Symptoms worse in heat of summer. Feels better in open air. There is great desire for open and for washing in cold water.
- ARSENIC ALBUM: Ringworm on scalp, hair falling out in patches. Skin dry rough. Skin looks white and pasty with cold and clammy perspiration. There is black vesicles and burning pain. Excessive exhaustion from least exertion.
- NATRUM CARB: Herpes circinatus. Skin dry, rough, and chapped. Dryness of skin with profuse sweat on least exercise or slightest labour.
- CLEMATIS: Insupportable itching from warmth of bed and after washing. Vesicular, scaly, scabby eruption with redness and burning.
- PHYTOLACCA: Skin itches and becomes dry, shrunken and pale. Popular and pustular lesions. Worse from warmth of bed; itching worse forepart of night, preventing sleep till midnight. Worse in damp weather and washing.
- GRAPHITES: Unhealthy skin. Every injury suppurates. Eruptions upon the ears, between fingers and toes and various parts of body from which a watery, transparent, sticky fluid oozes out.
- DULCAMARA: Vesicular eruptions with itching. Always worse in col, wet weather. Humid eruptions on face and palmer surface of hands. Worse at night, cold, and damp rainy weather. Thick, brown-yellow crusts, bleeding when scratched.
- RHUS TOX: Burning eczematous eruptions with tendency to scale formation. Itching intense. Worse in cold, wet, and rainy weather. Better in warm, dry weather and rubbing warm applications.
 Click here to Pay
Click here to Pay

Please send the screenshot at 880 090 0271
eMedicineHub Assistant
Always available • 24 / 7